What It Is, Why It Happens, and What You Can Do About It
Polycystic Ovarian Disease, commonly referred to as PCOD, is one of the most prevalent hormonal conditions affecting women of reproductive age in India. Despite how frequently it is diagnosed, there remains a great deal of confusion — and misinformation — surrounding what PCOD actually is, how it differs from PCOS, and what women can realistically do about it.
This article offers a comprehensive, clinically grounded overview of PCOD: its definition, causes, symptoms, potential complications, and the management strategies that have proven most effective. If you have been told you have PCOD, or suspect you might, this guide is designed to give you the clarity you need to take the right next steps.
What Is PCOD?
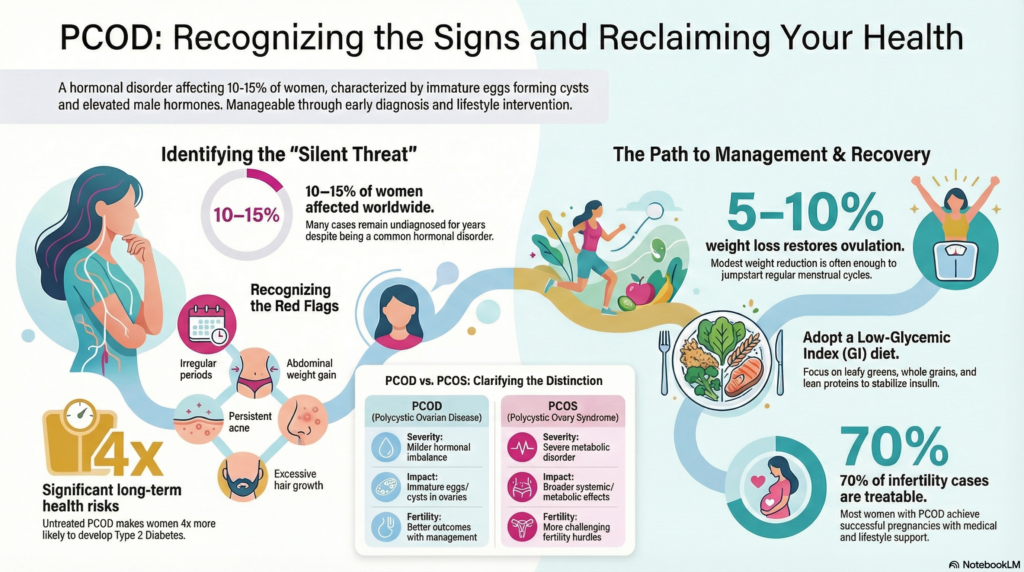
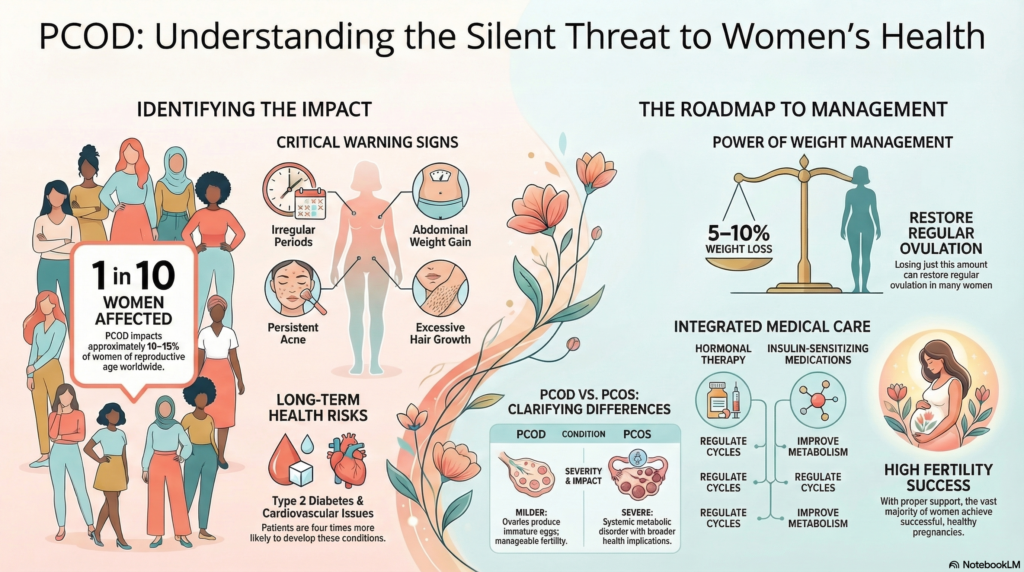
PCOD (Polycystic Ovarian Disease) is a condition in which the ovaries produce an abnormally large number of immature or partially mature eggs. Rather than fully maturing and being released through ovulation, these eggs accumulate within the ovaries and gradually develop into small, fluid-filled cysts. Over time, this process causes the ovaries to enlarge and disrupts their normal hormonal function.
The condition is primarily characterised by an excess production of androgens — hormones typically associated with male physiology — which interferes with the regularity of the menstrual cycle and can give rise to a range of associated symptoms.
PCOD vs. PCOS: Understanding the Difference
PCOD and PCOS (Polycystic Ovarian Syndrome) are frequently used interchangeably, but they are not identical conditions. Understanding the distinction matters, because it affects how the condition is managed and what outcomes women can expect.
Feature | PCOD | PCOS |
Nature | Lifestyle/hormonal disorder | Complex endocrine syndrome |
Severity | Generally milder | More severe and systemic |
Ovulation | Irregular but possible | Often absent |
Fertility Impact | Moderate; manageable | More significant |
Reversibility | Often reversible with lifestyle changes | Requires long-term management |
Metabolic Risk | Moderate | Higher (diabetes, cardiovascular) |
In clinical practice, PCOD is considered a milder, more lifestyle-driven condition. Many women with PCOD can restore normal ovarian function through diet, exercise, and weight management alone. PCOS, by contrast, involves a broader endocrine and metabolic disruption that typically requires more sustained medical intervention.
What Causes PCOD?
The precise cause of PCOD is not fully understood, but research points to a combination of genetic predisposition and environmental and lifestyle factors. The most commonly implicated contributors include:
Insulin Resistance
When the body’s cells do not respond efficiently to insulin, the pancreas compensates by producing higher levels of the hormone. Elevated insulin stimulates the ovaries to produce more androgens, which in turn disrupts ovulation and contributes to cyst formation. Insulin resistance is present in a significant proportion of women with PCOD.
Hormonal Imbalance
An imbalance between luteinising hormone (LH) and follicle-stimulating hormone (FSH) is commonly observed in PCOD. When LH levels are disproportionately high relative to FSH, the ovaries are stimulated to produce androgens rather than oestrogen, disrupting the normal follicular development process.
Genetic Factors
PCOD tends to run in families. Women with a mother or sister who has the condition have a significantly higher likelihood of developing it themselves, suggesting a heritable component — though the specific genes involved have not yet been definitively identified.
Sedentary Lifestyle and Poor Diet
A diet high in refined carbohydrates and sugars, combined with physical inactivity, contributes to insulin resistance and weight gain — both of which exacerbate hormonal imbalances. These lifestyle factors are particularly relevant given rising PCOD rates among young urban women in India.
Stress and Sleep Disruption
Chronic psychological stress elevates cortisol levels, which can adversely affect hormonal balance and contribute to menstrual irregularities. Poor sleep quality — which may be both a cause and consequence of PCOD — further compounds these effects.
Common Symptoms of PCOD
PCOD presents differently in different women. Some experience a cluster of pronounced symptoms; others have only mild or intermittent complaints. The most commonly reported symptoms include:
- Irregular, delayed, or missed menstrual periods
- Heavy or prolonged menstrual bleeding when periods do occur
- Excess facial and body hair (hirsutism), particularly on the chin, upper lip, and chest
- Persistent acne or oily skin that does not respond well to standard treatments
- Unexplained weight gain, particularly concentrated around the abdomen
- Difficulty losing weight despite dietary efforts and exercise
- Scalp hair thinning or male-pattern hair loss
- Darkening of skin in skin folds — neck, underarms, groin (acanthosis nigricans, associated with insulin resistance)
- Fatigue and low energy levels
- Mood changes, anxiety, or depressive symptoms
- Difficulty conceiving due to infrequent or absent ovulation
It is important to note that many of these symptoms overlap with other gynaecological and endocrine conditions. A proper clinical assessment — including a pelvic ultrasound, hormonal blood panel, and medical history review — is essential for an accurate diagnosis.
Experiencing irregular periods or other PCOD symptoms? Our gynaecologist in Attapur, Hyderabad offers comprehensive hormonal assessments and personalised PCOD management plans. Book a consultation today.
Potential Complications if Left Unmanaged
When PCOD is not identified and addressed in a timely manner, it can lead to a range of longer-term health complications:
Infertility
Irregular or absent ovulation is the primary mechanism by which PCOD affects fertility. While many women with PCOD do conceive — sometimes without medical assistance — those who do not ovulate regularly may require intervention such as ovulation induction or assisted reproductive techniques.
Type 2 Diabetes
The insulin resistance that underlies many cases of PCOD significantly raises the risk of developing Type 2 diabetes, particularly if it is not addressed through lifestyle modifications. Women with PCOD are advised to undergo regular blood glucose monitoring.
Endometrial Hyperplasia
Prolonged periods without ovulation mean the uterine lining (endometrium) is not shed regularly. Continuous oestrogen exposure without the balancing effect of progesterone can cause the endometrium to thicken abnormally — a condition known as endometrial hyperplasia, which, if untreated, increases the risk of endometrial cancer.
Cardiovascular Risk
Elevated androgens, insulin resistance, obesity, and dyslipidaemia (abnormal cholesterol levels) collectively raise cardiovascular risk in women with untreated PCOD. This risk becomes more pronounced after menopause.
Mental Health Impact
The visible symptoms of PCOD — weight gain, acne, excess hair growth — can significantly affect self-esteem and body image. Combined with the hormonal drivers of mood disruption, women with PCOD have a higher prevalence of anxiety and depression than the general population. These aspects of the condition deserve clinical attention alongside the physical symptoms.
How Is PCOD Diagnosed?
There is no single definitive test for PCOD. Diagnosis is typically based on a combination of the following:
- Clinical history: menstrual pattern, symptom onset, family history
- Physical examination: signs of hyperandrogenism such as hirsutism or acne
- Pelvic ultrasound: to assess ovarian morphology and identify the characteristic appearance of multiple small follicles
- Hormonal blood tests: LH, FSH, testosterone, prolactin, thyroid function, fasting insulin, and blood glucose
- BMI and waist circumference measurement
It is important to rule out other conditions — such as thyroid disorders, hyperprolactinaemia, or congenital adrenal hyperplasia — that can mimic PCOD symptoms before confirming the diagnosis.
Managing PCOD: What Actually Works
The encouraging reality about PCOD — in contrast to PCOS — is that it responds well to lifestyle intervention. Many women experience a significant reduction in symptoms and restoration of regular menstrual cycles through the following approaches:
Weight Management
Even a modest reduction in body weight of 5 to 10 percent has been shown to improve hormonal balance, restore ovulation, and reduce androgen levels in women with PCOD. Weight loss is most effectively achieved through a combination of dietary changes and structured physical activity.
Dietary Modifications
A low glycaemic index (GI) diet — emphasising whole grains, legumes, vegetables, lean proteins, and healthy fats while minimising refined carbohydrates and sugars — helps reduce insulin resistance. Avoiding processed foods, sugary beverages, and excessive dairy may also be beneficial for some women.
Regular Physical Activity
A minimum of 150 minutes of moderate-intensity aerobic exercise per week, combined with strength training, helps improve insulin sensitivity, support weight management, and reduce androgen levels. Consistent exercise has also been shown to improve mood and reduce stress.
Stress Management
Practices such as yoga, meditation, and adequate sleep hygiene have been shown to lower cortisol levels and support hormonal balance. For women experiencing clinical anxiety or depression alongside PCOD, psychological support should be considered as part of the overall management plan.
Medical Treatment (When Required)
Depending on the severity of symptoms and the woman’s reproductive goals, a gynaecologist may recommend:
- Oral contraceptive pills: to regulate menstrual cycles and reduce androgen levels
- Metformin: to improve insulin sensitivity
- Anti-androgen medications: to manage hirsutism and acne
- Ovulation induction agents: for women trying to conceive
Medical treatment is always individualised and based on the patient’s specific symptom profile, reproductive intentions, and metabolic health status.
Frequently Asked Questions
Can PCOD be cured permanently?
PCOD is not considered curable in the traditional sense, but it is highly manageable. Many women achieve complete symptom resolution and regular menstrual cycles through sustained lifestyle changes. Unlike PCOS, PCOD does not always require lifelong medical management.
Does PCOD mean I cannot get pregnant?
Not at all. PCOD affects ovulation, which can reduce fertility, but the majority of women with PCOD are able to conceive — either naturally or with appropriate medical support. Early diagnosis and management significantly improve fertility outcomes.
Is PCOD common in India?
Yes. Estimates suggest that PCOD affects between 20 and 30 percent of women of reproductive age in India, with particularly high rates observed among urban populations. Sedentary lifestyles, high-carbohydrate diets, and rising stress levels are believed to be contributing factors.
At what age does PCOD typically develop?
PCOD most commonly develops during adolescence or early adulthood — often appearing shortly after the onset of menstruation. However, it can be diagnosed at any age during the reproductive years and is sometimes first identified when a woman is investigated for difficulty conceiving.
When should I see a gynaecologist for PCOD?
You should consult a gynaecologist if you experience irregular or absent periods, unexplained weight gain, excess facial hair, persistent acne, or difficulty conceiving. Early assessment allows for timely management before complications develop.
Conclusion
PCOD is a common but manageable hormonal condition that affects a significant proportion of women across India. While it can disrupt menstrual regularity, fertility, and overall well-being, it responds remarkably well to lifestyle intervention — particularly when identified early.
If you are experiencing symptoms consistent with PCOD, the most important step you can take is to seek a proper clinical assessment. Self-diagnosis and self-treatment — particularly through unverified supplements or restrictive diets — can delay appropriate care and allow complications to develop.
A qualified gynaecologist can evaluate your symptoms comprehensively, confirm the diagnosis, and work with you to develop a management plan that is both clinically sound and tailored to your individual circumstances and goals.